
Please visit Melbourne Gallbladder Centre
Keyhole Gallbladder Removal Surgery (Cholecystectomy)
Laparoscopic or keyhole removal of the gall bladder was one of the first procedures to utilise the laparoscopic surgical technique. The procedure has been in use since 1993 in Australia, with many thousands of the procedures being performed. The benefits of the laparoscopic technique include less pain, shorter hospital stays, faster recovery times, fewer post operative small bowel obstructions, and fewer wound infections.
Mr Steven Karametos's standard of care for gallstone disease is laparoscopic cholecystectomy, which is a minimally invasive surgical option for removing the gallbladder. This is a very safe operation.
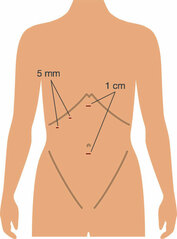
The laparoscopic removal of the gall bladder (cholecystectomy) is performed under general anaesthetic so the patient must be in reasonable health. Mr Karametos makes three or four cuts in the abdominal wall, each of these cuts is generally no more than 1 cm in length. The first is in the umbilicus. The abdomen is then blown up with carbon dioxide (CO2) gas. This lifts the abdominal wall upwards, and gives the surgeon space to operate. After that, telescope attached to a tiny video camera is introduced and the abdominal contents inspected. The gall bladder is readily located and is grasped with forceps. It is freed from attachments to the liver. A small tube, the cystic duct, connecting the gall bladder to the bile duct is dissected free of the fatty tissue that encases it and a catheter inserted into it. Dye is injected down this and an x-ray of the main bile duct, which takes bile from the liver to the intestine, is taken. This is to confirm that no gallstones have entered the bile duct where they could cause a blockage leading to obstructive jaundice. Once the Xray has been completed, the cystic duct and the little artery feeding the gall bladder are clipped with little metal clips and divided. The gallbladder is then dissected away from the liver and removed through the small incision beneath the umbilicus. It is like a small bag that passes through the little incision once the stones and bile have been emptied out of it.
The operation usually takes 30 to 90 minutes. At the end of the operation the carbon dioxide gas is let out. Laparoscopic cholecystectomy is preferable to open surgery because the cuts made are much smaller, postoperative pain is less, hospital stay is shorter, and the return to normal activity much quicker.
In a small number of patients (less than 1 percent), it may not be possible to remove the gallbladder by the keyhole method because of inflammation and scarring around the gallbladder, or the anatomy of the structures is not clear. The risk of conversion to open surgery is higher if you have undergone previous operations on your abdomen or suffered from peritonitis. Other reasons for open surgery include a history of bleeding disorders and with pregnancy.
If laparoscopic cholecystectomy is not possible, Mr Karametos may consider converting the operation to an open surgical operation through a traditional surgical incision. What is done inside is exactly the same, but there is a bigger wound, and therefore a longer convalescence, usually 3-5 days.
Mr Steven Karametos's standard of care for gallstone disease is laparoscopic cholecystectomy, which is a minimally invasive surgical option for removing the gallbladder. This is a very safe operation.
The laparoscopic removal of the gall bladder (cholecystectomy) is performed under general anaesthetic so the patient must be in reasonable health. Mr Karametos makes three or four cuts in the abdominal wall, each of these cuts is generally no more than 1 cm in length. The first is in the umbilicus. The abdomen is then blown up with carbon dioxide (CO2) gas. This lifts the abdominal wall upwards, and gives the surgeon space to operate. After that, telescope attached to a tiny video camera is introduced and the abdominal contents inspected. The gall bladder is readily located and is grasped with forceps. It is freed from attachments to the liver. A small tube, the cystic duct, connecting the gall bladder to the bile duct is dissected free of the fatty tissue that encases it and a catheter inserted into it. Dye is injected down this and an x-ray of the main bile duct, which takes bile from the liver to the intestine, is taken. This is to confirm that no gallstones have entered the bile duct where they could cause a blockage leading to obstructive jaundice. Once the Xray has been completed, the cystic duct and the little artery feeding the gall bladder are clipped with little metal clips and divided. The gallbladder is then dissected away from the liver and removed through the small incision beneath the umbilicus. It is like a small bag that passes through the little incision once the stones and bile have been emptied out of it.
The operation usually takes 30 to 90 minutes. At the end of the operation the carbon dioxide gas is let out. Laparoscopic cholecystectomy is preferable to open surgery because the cuts made are much smaller, postoperative pain is less, hospital stay is shorter, and the return to normal activity much quicker.
In a small number of patients (less than 1 percent), it may not be possible to remove the gallbladder by the keyhole method because of inflammation and scarring around the gallbladder, or the anatomy of the structures is not clear. The risk of conversion to open surgery is higher if you have undergone previous operations on your abdomen or suffered from peritonitis. Other reasons for open surgery include a history of bleeding disorders and with pregnancy.
If laparoscopic cholecystectomy is not possible, Mr Karametos may consider converting the operation to an open surgical operation through a traditional surgical incision. What is done inside is exactly the same, but there is a bigger wound, and therefore a longer convalescence, usually 3-5 days.
Diet For Gallstone Patients
If certain fatty foods have triggered your attacks of pain, you should avoid those. In general, you will be better off if you adopt a low fat diet. This will not get rid of your gallstones, but may reduce the severity and frequency of your attacks of pain. Here are some tips:
- Eat less
- Eat only when hungry; stop eating when you are full
- Eat mainly plants; less meat
- Eat fish or poultry in preference to red meat, as red meat contains more fat
- Avoid dairy and egg
- Eat home cooked food (where you can control what goes in, rather than purchased or processed foods)
- Trim all fat and skin off meat when cooking
- When cooking vegetables or meat, try to boil, steam, grill, bake or shallow-fry in a non-stick pan rather than deep-fry or cook in a rich sauce
- When baking cakes, half of the butter can usually be replaced by zero fat yogurt
- When buying food, look at the fat content and opt for low fat version
- Cut down on oily foods, such as deep-fried food, cheesy dishes
For A Gallbladder Attack
For a mild attack of biliary pain, try Paracetamol or Ibuprofen (assuming you have no allergies to either of these drugs and no asthma) as well as some anti-acid medication (for example Gaviscon or Omeprazole). Buscopan may help too. If the pain is very severe to start with or does not settle with these medications, please seek urgent medical help. Please remember - just because you have gallstones does not mean you cannot have other problems like angina or acid reflux.
Inflamed Gallbladder & Gallbladder Surgery
Mr Karametos will discuss this with you during consultation. If your attack of acute cholecystitis has started only in the last 7 days, and the diagnosis has been made promptly, then it may be reasonable to proceed immediately to an operation. But with each passing day, the tissues around the gall bladder can become more inflamed and “sticky”, and it may then be safer to wait for 4-6 weeks and let the inflammation settle before doing the cholecystectomy.
Gallbladder Surgery During Pregnancy
Here are a few general guidelines about surgery during pregnancy (other than obstetric operations):
- Elective (non-urgent) operations that can be safely postponed, should be postponed until after delivery.
- If possible, non-urgent surgery should be performed in the second trimester (i.e. months 4,5 and 6).
- A pregnant woman should never be denied emergency surgery for life-threatening conditions, regardless of where she is in the course of her pregnancy.
Before Gallbladder Surgery
Prior to your gallbladder surgery, Mr Karametos will spend time with you to explain the procedure and complete Surgery Consent Form during consultation. Our office staff will then provider you with the general Pre/ Post- Operative Instructions to take home. Please do read this document carefully before the surgery, you may also download a copy HERE. Please feel free to call us within business hours on (03) 9857 3600 should you have any other questions.
Recovery After Gallbladder Surgery - In Hospital
You will wake up feeling drowsy in the operating theatre’s recovery area. You will then be taken back to the ward. There will be some pain and sickness for 12 to 24 hours, but you will be given medications for this. Some bruising and slight oozing of blood around the cuts is normal. Once you are fully awake, you will be encouraged to walk around and drink fluids. You should then be able to eat something light a few hours later. Ask Mr Karametos about the care of your wounds. In most instances your cuts will be closed with glue or with self-dissolving stitches under the skin. Waterproof dressings allow for short showers after the surgery. Some pain and mild bruising around the wounds is normal.
Diet After Gallbladder Surgery
Surprisingly, removal of the gallbladder seems to have no effect on the digestive process in the vast majority of patients who undergo this operation. The bile trickles steadily into the gut and helps digest the fatty foods. The digestive system just adapts to the absence of the gallbladder. You should be able to continue eating normally after the operation. You do not need to modify your diet because your gallbladder has been removed.
Diarrhoea After Gallbladder Surgery
A small number of people develop frequent loose, watery stools after surgery to remove their gallbladders. In most cases, the diarrhoea resolves soon afterwards. Rarely, it may last longer. The cause of diarrhoea after gallbladder removal is not known. It may be due to more bile acids entering the intestine and acting as a laxative. Please contact Mr Karametos's rooms and we may advises you to try anti-diarrhoeal medications and cut down on foods that can worsen diarrhoea in general, including dairy products, very greasy or sweet foods, and caffeine.
Complications
Every operation inevitably carries a small element of risk, but your surgeon, anaesthetist and nurses will take great care to prevent complications. The likelihood of complications after an operation to remove the gall bladder is very low. There some risks associated with the general anaesthetic, including pneumonia, heart problems, and blood clots in the leg veins and lungs.
If you find any redness or discharge in the wound, get an unusual amount of pain, develop a fever, or develop jaundice (your eyes and skin look yellow), do contact Mr Karametos's rooms or the hospital, as these may be signs of a wound infection or other complications.
If you find any redness or discharge in the wound, get an unusual amount of pain, develop a fever, or develop jaundice (your eyes and skin look yellow), do contact Mr Karametos's rooms or the hospital, as these may be signs of a wound infection or other complications.
Post- Cholecystectomy Syndrome
Around 95% of patients are well and free of symptoms after a cholecystectomy. In a small number of patients the old symptoms may persist, or new symptoms may develop. The term post-cholecystectomy syndrome is sometimes used to describe this situation. The first thing to consider is were the initial symptoms caused not by the gallstones but by some other problem that was not picked up (such as acid reflux or a peptic ulcer or chronic pancreatitis)? Further tests may be required to diagnose these, for example an endoscopy. The second possibility is that there may be a gallstone that has been left behind, perhaps in the bile duct. Blood tests and an ultrasound or MRCP scan can clarify this, and an endoscopic procedure (ERCP) can usually be done to remove the stone.
These are rare problems, but if and when they do occur, you need to have a detailed discussion with Mr Karametos. A careful history and examination, and the correct tests, can often help find the underlying cause, which can then be treated.
These are rare problems, but if and when they do occur, you need to have a detailed discussion with Mr Karametos. A careful history and examination, and the correct tests, can often help find the underlying cause, which can then be treated.
Recovery Timeline After Gallbladder Surgery
Usually patients can go home the same or next day post-operatively. One week off work is sufficient for sedentary workers. For those who do heavy lifting, Mr Karametos advises three weeks off to allow the umbilical wound to settle and strengthen. If you want to go to the gym, wait for 2 weeks, and then re-start gently. You will need 5 days before returning to driving. When recovering from a gallbladder operation, If doing something hurts your tummy, then stop doing it.
Operating Video
Mr Karametos preforms a Laparoscopic Cholecystectomy of Gangrenous Gallbladder (Gallbladder & Gallstones Removal).
Further Reading
Please read Cholecystectomy- Patient Education (ref: American College of Surgeons) for a comprehensive overview of this procedure, which includes surgery preparation and recovery after the gallbladder operation.



